PATIENT
PHYSICIANS
The main function of the circulatory system is the delivery of oxygen and nutrients to the cells of the organism. For this reason, each cell has to be close to the nearest vessel and the distance cannot be more than 200 microns. In case of hypoxia, a condition when cells are deprived of oxygen, new vessel growth is necessary to enhance local blood flow and as a consequence, the influx of nutrients and oxygen. Angiogenesis is the compensatory mechanism aimed at improving perfusion in presence of tissue hypoxia via formation of the new blood vessel from already existing ones. The main trigger for that mechanism is hypoxia activated molecular factor HIF-1 (Hypoxia Induced Factor-1). Being inactive in normoxic conditions, HIF-1 in hypoxic conditions stimulates the expression of key pro-angiogenic molecular factors, such as VEGF (Vascular Endothelial Growth Factor), which leads to angiogenesis.
Formation of the vessels can be divided into three main stages: branch initiation with formation of a branch point in the vessel wall, elongation of vessel tubular structures (re-organisation of endothelial cells to form tubules with a central lumen), and «maturation» of the vascular wall with the following interconnection of the new tubules to form a network.
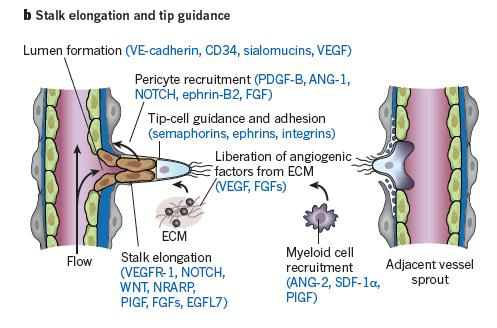
Branch Initiation. During the first stage, a loss of intercellular junctions between endothelial cells (EC) occurs under the action of angiogenic growth factors, which leads to the formation of the basis of the capillary wall. Dissociation of pericytes (cells of connective tissue) supports the activity of the EC, regulate the capillary lumen, and increases the permeability of vessels. VEGF increases the EC proliferation and the expression of matrix metalloproteinases (MMPs), which is accompanied by the degradation of the basement membrane of the capillary and penetration of blood plasma into the surrounding extracellular matrix (ECM) with its subsequent degradation. Under these conditions EC, which actively proliferate, migrate beyond the basal membrane. The first cells that migrate into the ECM form the growth cone («tip» -cells). The «tip»-cells lead the migrating endothelial cells according to the concentration gradient of the angiogenic growth factors in the direction of ischemia. Actively dividing EC migrate along with them, filling the channel space formed by the «tip» cells.

Elongation of the vessel tubular structure. During the second stage of the angiogenesis new vessel growth cone is promoted towards ischemia with simultaneous formation of tubular structure and re-organisation of endothelial cells to form tubules with a central lumen. After reaching the growth cone at the other end of the capillary this stage is finalized by the formation of «immature» vessel.
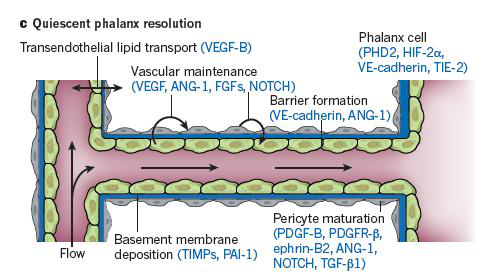
The stabilization of the vascular wall. The final stage represents the «maturation» of the vascular wall with the following interconnection of the new tubules to form a network. The most important cellular elements at this stage are pericytes which migrate to the newly formed vessels together with the EC. Restoration of tissue perfusion due to the increased capillary density leads to the normal oxygen level (normoxia), inactivation of the transcription factor HIF-1, and reversible inhibition of other angiogenic factors.
There are many factors which impair angiogenesis such as smoking, atherosclerosis, age-related dysfunction of the circulatory system, hypertension, diabetes etc.. As a result, the mechanisms of growth and formation of blood vessels are impaired due to the disruption of the delicate relationship between the molecular signaling systems in response to hypoxia via the activity of trigger factors. One of the new concepts aimed at correcting ischemia by restoration of compensatory mechanisms is therapeutic angiogenesis.
Therapeutic angiogenesis comprises a group of methods, aimed at compensating for the low perfusion in ischemic tissues via induction of a natural process of vessel formation and growth. The methodological basis for therapeutic angiogenesis can be divided into three main areas: 1) the use of recombinant proteins which induce angiogenesis, 2) gene therapy, and 3) stem cells.
The first method is the use of recombinant angiogenic growth factors. Within this framework, the induction and regulation of angiogenesis is carried out by administering intravenously, intramuscularly or elsewise a single agent or a combination of factors, proteins, and therapeutic agents exerting a direct action via interaction with receptors on the target cells. Numerous experiments have shown that the use of recombinant angiogenic growth factors, such as fibroblast growth factor (FGF,) and vascular endothelial growth factor (VEGF) contributed to neovascularization of ischemic tissues, however, difficulties arose with the establishment and maintenance of their effective concentration in the tissues.
Another option is gene therapy which is mostly focused on the study of VEGF-165, FGF-1, FGF-2, and hepatocyte growth factor (HGF).
Therapeutic angiogenesis with gene therapy is accomplished by administering a gene construct comprising vector with a gene encoding a protein with angiogenic properties. British Advisory Committee for gene therapy in 2004 gave the following definition of gene therapy: « «The deliberate introduction of genetic material into human somatic cells for therapeutic, prophylactic or diagnostic purposes.».» A gene construct contains a single gene or a combination of genes . The choice of the genes is determined by the desired therapeutic effect in relation to a particular disease. Monogenic diseases are a promising application target for gene therapy, which will compensate for the defective genes. Different methods and delivery systems (vectors) are used to implement the delivery of genetic information into the cell (transfection). Such vectors are divided into viral and non-viral. In the first case, genetically modified viruses are used as carriers of genetic information. In the case of non-viral vectors, gene constructs are based on a small double-stranded molecule of plasmid DNA,. Transfection is followed by the gene expression, which eventually leads to the process of angiogenesis. The target cells become a «bioreactor» producing proteins and exerting a sustained therapeutic effect.
Thus, the main difference in therapeutic angiogenesis based on the use of recombinant proteins and gene therapy is that in the latter case a gene construct transfer leads to the expression of a therapeutic gene , which increase the endogenous production of an angiogenic growth factor.
Another trend in therapeutic angiogenesis is the use of cell therapy. The idea of the use of cell therapy is based on the concept of progenitor cells contributing to the formation of vascular wall and inducing the vascular growth. Paracrine cellular activity is also taken into account, causing a local increase in the concentration of cytokines, growth factors, and other signaling molecules. Success rate depends on the source of progenitor cells and the degree of differentiation. Different stem cells can be used for cell therapy: embryonic stem cells (ESC), induced pluripotent stem cells (iPSC), fetal and amniotic stem cells, and hematopoietic adult stem cells. Various administration routes may apply.


