PATIENT
PHYSICIANS
Treatment of patients with atherosclerotic peripheral arterial disease remains an unsolved problem of modern angiology. Great hopes are vested in therapeutic angiogenesis, an innovative method of treatment. The developers of the first-in-class drug Neovasculgen® launched a new generation of genetic pharmacological drugs based on nucleic acids (plasmid DNA) with a gene encoding the synthesis of growth factors involved in angiogenesis, which provides for the blood vessel growth.
Treatment of the ischemic lesions of the lower limbs is a challenging issue for the specialists in cardiovascular medicine. The prevalence of the lower limb ischemia in the population aged 50 or over is 5-8%, and in the presence of risk factors such as hyperlipidemia, smoking, hypertension or diabetes increases up to 30%. The most frequent cause of lower limb ischemia is atherosclerosis (about 90% of all patients).
Depending on the severity of the disease according to the classification introduced by Fontaine in modification by acad. A.V. Pokrovsky (Fig. 1) lower limb ischemia is divided into several stages.
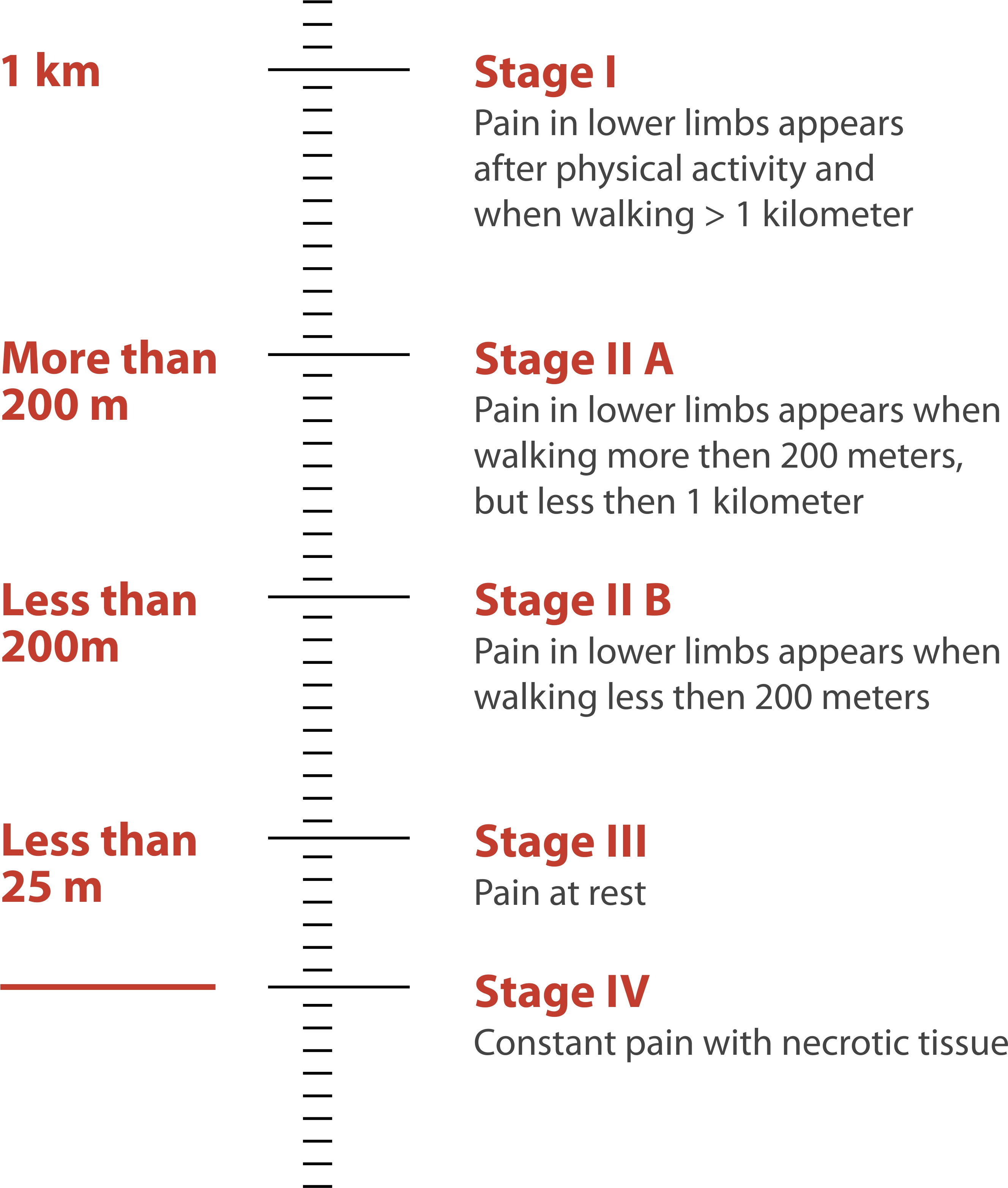
Fig 1. Classification of lower limb ischemia by Pokrovsky-Fontaine.
Main symptoms of chronic lower limb ishemia include:
pain when walking that is relieved with rest — «intermittent claudication»;
bluish, cold skin in the affected limb;
muscle wasting/muscle asymmetry;
cold feet;
dry skin in the affected leg;
poor nail and hair growth in the affected limb.
The prognosis regarding the limb salvage depends on the location and nature of arterial lesions, extent and severity of ischemia of the extremities, and the possibilities to restore arterial perfusion. The prognosis regarding survival depends on the severity of limb ischemia and the severity of co-existing comorbidities. Annually CLI causes limb amputation in 35-40 thousand people among Russian population.
In critical limb ischemia (CLI) the symptoms included:
pain at rest;
loss of tissue and ulcerous/necrotic legions in the affected leg.
Prognosis in patients with CLI is poor: approximately one half of CLI patients with an established diagnosis are subject to limb revascularization, a quarter of the patients receive conservative treatment, while the rest are subjected to amputation major amputation (Figure 2).

Figure 2.The fate of patients with critical limb ischemia.
As a result, by the end of the first year after establishing a CLI diagnosis limb salvage is achieved only in 45% of patients, about 30% of patients undergo a major amputation, and 25% of patients die.
The effectiveness of conservative treatment is low; limb salvage is achieved only in 40% of patients treated conservatively within the first 6 months, 20% of patients die, the rest are subjected to a major amputation (Fig. 3)

Figure 3. The results of conservative treatment of CLI 6 months after diagnosis.
Aortoiliac occlusion (Type I and II).
Type I Aortoiliac occlusions are rare (10-15%) and are characterized by the presence of atherosclerotic lesions in the distal aorta and the common iliac arteries. Normally this type of lesions occurs in 35-55 year old patients who are heavy smokers. Hypertension and diabetes mellitus are rare among these patients, however hyperlipidaemia is often present. The patients’ complaints include intermittent claudication with pain in the proximal limb segments, including the hip and thigh muscles, and in the calf muscles in later stages of the disease . In some cases, men demonstrate a tetralogy of symptoms including intermittent claudication, impotence, muscle atrophy, and lack of pulses in the femoral arteries, which is called Leriche syndrome. Type II lesions (20% of cases) are present in the aortoiliac segment and the external iliac artery. Vascular imaging is needed to identify the type of lesion.
Aortoiliac and femoropopliteal lesions (Type III)
A combination of aortoiliac and femoropopliteal lesions is found in the majority (66%) of patients with intermittent claudication (Type III). Such lesions usually occurs in patients with multiple risk factors such as smoking, hypertension, hyperlipidemia, and, sometimes, diabetes arising in adulthood. Typically, the symptoms of ischemia are more severe in patients with type III disease as compared with those with isolated aortoiliac or femoropopliteal lesions. Such type of the disease often progresses to critical limb ischemia, i.e. pain at rest, ischemic ulcers and/or gangrene.
Isolated femoropopliteal lesions (Type IV).
Isolated femoropopliteal lesions are usually accompanied by the symptoms of intermittent claudication. This type of lesions is frequently found in elderly patients (50-70 years old and over), often suffering from hypertension, type II diabetes, and coronary and/or carotid artery disease. Popliteal and foot pulses are absent in type IV lesions. Exercise may improve the symptoms of intermittent claudication in such patients in the absence of concomitant aortoiliac lesions. Therefore, these patients are subjected to conservative therapy, which allows for long-term limb salvage in patients older than 60 years of age. The probability of amputation is low — 2-12% within 10 years. The five-year survival rate is 70-80%, and only 10% of these patients will require surgical revascularization
Isolated occlusion of femoral popliteal segment (Type V)
The patients with type V lesions especially those of 65 years of age and older are at the highest risk of limb loss due to poor long-term outcomes of revascularization at the level of the tibial segment. This type of lesion is often seen in patients with diabetes, lipid disorders, and smokers. All these factors contribute to the progression of the disease. In some of these patients despite the patency of aortoiliac and femoropopliteal segments, diffuse and severe lesions occur in the tibial arteries.
Therapeutic angiogenesis can be used in patients with both type IV and V lesions. In addition, according to the statistics, about 20-30% of patients with lower limb ischemia cannot be subjected to surgical intervention due to the type of atherosclerotic lesion, or have neurological disorders or other severe concomitant pathology. In such patients a primary amputation is often the only treatment option. Therapeutic angiogenesis as an alternative treatment strategy may be considered for the treatment of such patients.


